Graft Selection in Knee Arthroscopy: Options, Outcomes & Considerations
Knee arthroscopy has revolutionized orthopaedic surgery, transforming how we treat ligament injuries. Central to the
success of Anterior Cruciate Ligament (ACL) and Posterior Cruciate Ligament (PCL) Reconstruction is the use of
grafts—biological tissues used to replace the damaged ligament. The choice of graft and the method of harvesting it
are critical decisions that directly impact patient recovery, long-term function, and the ability to return to
sport.
Why Graft Harvesting is Important
In ligament reconstruction, the torn ligament is replaced with a biological graft that acts as a scaffold for new
ligament formation. An ideal graft should:
- Provide adequate tensile strength
- Allow secure fixation
- Promote biological incorporation
- Cause minimal donor site morbidity
- Facilitate early rehabilitation
Proper harvesting ensures graft integrity, appropriate length and diameter, and minimal complications.
Choosing the Right Graft
Graft selection depends on:
- Patient age
- Activity level
- Sport type
- Previous surgeries
- Surgeon expertise
- Revision vs primary surgery
For example:
- Young competitive athletes → BPTB or Quad tendon
- Cosmetic concerns or kneeling occupation → Hamstring
- Revision cases → Quadriceps tendon or allograft
Categories of Grafts
Grafts for ACL and PCL surgery generally fall into two main categories:
- 1.Autografts:Tissue harvested from the patient’s own body. These remain the most popular choice
for primary (first-time) reconstructions due to excellent biological healing.
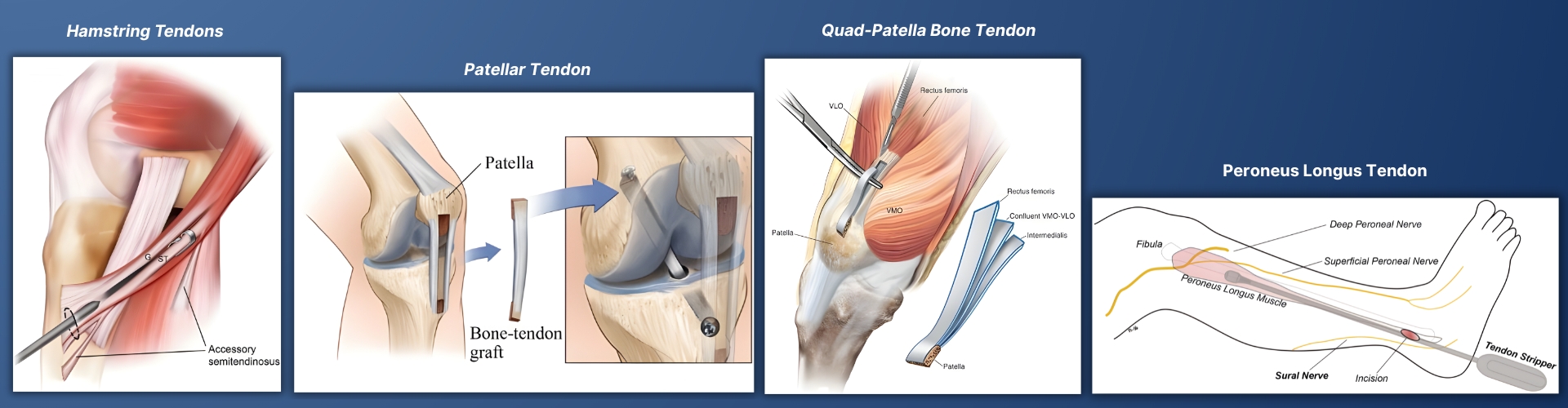
The four most commonly used
autografts are the Bone-Patellar tendon-bone (BPTB), Hamstring tendon, Quadriceps tendon, and the Peroneus
Longus tendon.
- 2.Allografts:Tissue taken from a deceased donor. These are valuable in revision surgeries, multi-ligament injuries, or for older, less active patients.
- Tibialis anterior
- Achilles tendon
- No donor site morbidity
- Shorter operative time
- Higher cost
- Slightly higher failure rate in young athletes
- Slower biological incorporation
- Ideal ACL graft diameter: ≥8mm
- Smaller grafts have higher re-tear risk
- Must accommodate femoral and tibial tunnel lengths
- Adequate intra-articular portion required
- Avoid excessive handling
- Prevent tendon fraying
- Proper bleeding control reduces post-op pain and hematoma
1. Autograft Options: A Detailed Comparison
Summary Table: Autograft Options for ACL/PCL Reconstruction
|
|
Bone-Patellar Tendon-Bone (BPTB) |
Hamstring Tendon (ST/G) |
Quadriceps Tendon (QT) |
Peroneus Longus (PLT) |
|
Harvest Site |
Anterior knee (patella & tibia) |
Medial proximal tibia (pes anserinus) |
Superior pole of patella (anterior thigh) |
Lateral ankle (behind lateral malleolus) |
|
Healing Type |
Bone-to-bone (fastest) |
Tendon-to-bone (slower) |
Tendon-to-bone (or bone-to-bone) |
Tendon-to-bone |
|
Primary Advantage |
Excellent graft stability and fixation |
High tensile strength, smaller knee incision |
Large cross-section, high strength, low donor-site pain |
Larger diameter, predictable size, no knee morbidity |
|
Primary |
Donor-site morbidity: Anterior knee pain, kneeling pain, risk of patellar fracture |
Possible knee flexion weakness, unpredictable size, thigh atrophy |
Less historical long-term data |
Potential ankle morbidity (eversion weakness, nerve issues) |
|
Graft Length |
~7-9 cm (including bone plugs) |
Variable, often 8-12 cm (folded) |
~8-10 cm |
Excellent length (24-32 cm typical) |
|
Graft Diameter |
9-11 mm (with bone plugs) |
Variable (often 7-8.5 mm) |
8-10 mm |
Larger (7.5-9.5 mm average) |
2. Allografts (Donor Tissue)
Allografts are obtained from cadaveric donors and processed in tissue banks.
Common types:
Advantages:
Limitations:
Key Surgical Considerations in Graft Harvesting
✔ Graft Diameter
✔ Graft Length
✔ Preservation of Tissue Integrity
✔ Hemostasis
References
https://link.springer.com/article/10.1186/s40634-023-00600-4